

For hospital facility directors, the Air Handling Unit (AHU) room is often treated as a mechanical expense. It is a costly miscalculation with clinical consequences. To a Care Quality Commission (CQC) inspector or an HTM 03-01 auditor, that plant room is your hospital’s ultimate clinical liability.
When a hospital fails an airborne infection-control audit, the root cause is rarely the clinical staff. It is usually “Phantom Bypass.” These are the microscopic casing leaks in standard commercial AHUs, allowing untreated air to bypass HEPA filters entirely.
This guide strips away the standard HVAC feature-dump to focus on what actually matters to your hospital’s operations: solving critical compliance failures, proving ROI on hygienic upgrades, and securing the sterile boundary of your high-risk wards.
What Matters: Outcomes Over Airflow
You do not buy a medical-grade AHU to cool the building. You invest in it to achieve three non-negotiable outcomes: legal compliance, infection control, and energy decarbonisation.
Real Use Cases: Where the AHU Room Dictates Clinical Safety
Standard air conditioning serves an entire building. The mathematical engineering of an AHU room in a hospital serves specific clinical zones.
Source: ASHRAE (American Society of Heating, Refrigerating and Air-Conditioning Engineers)
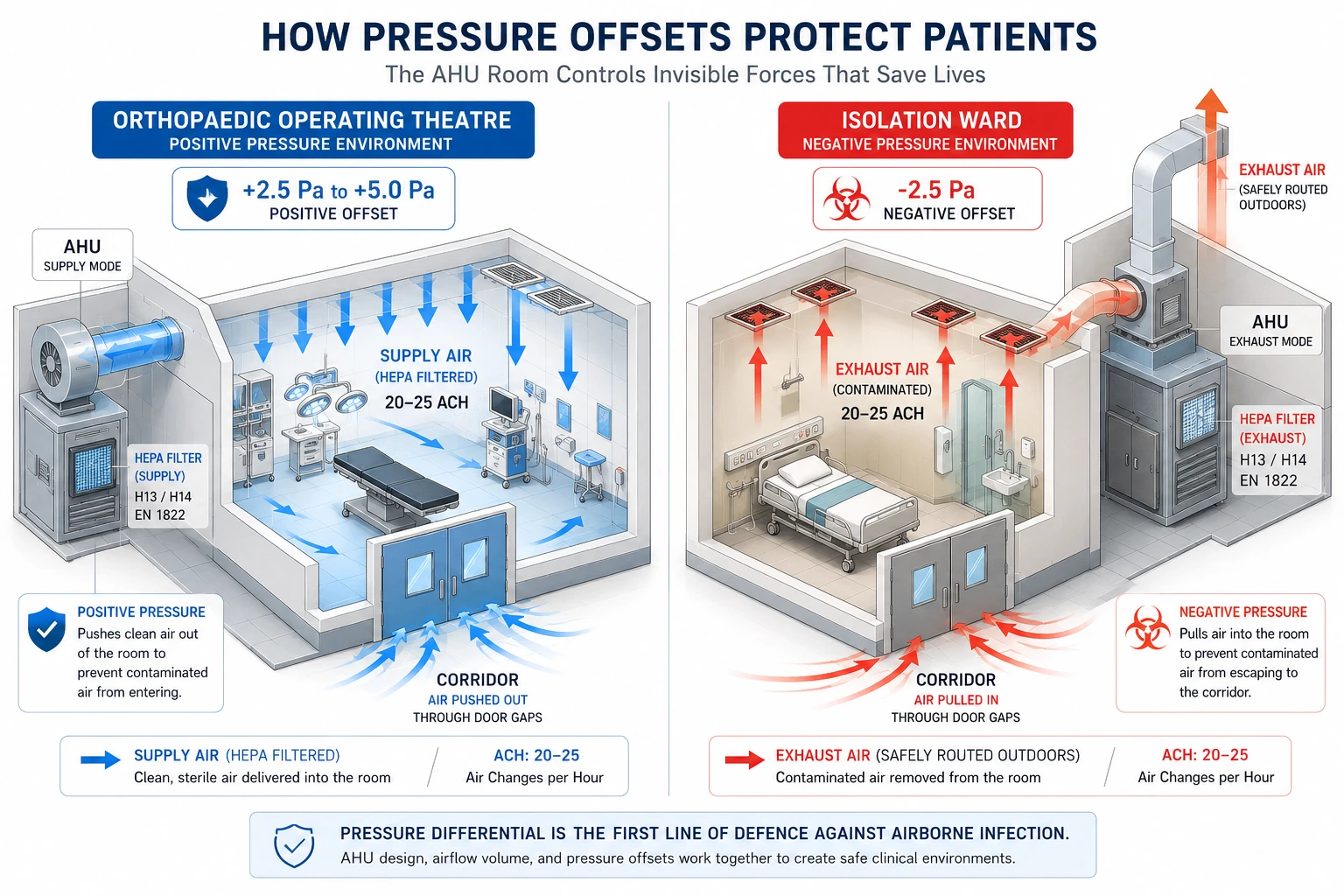
Use Case 1: The Orthopaedic Operating Theatre (Positive Pressure)
- The Problem: Deep-tissue surgeries (such as joint replacements) are highly susceptible to airborne bacterial contamination. Corridor air entering the theatre can be catastrophic.
- The AHU Outcome: The AHU maintains a continuous positive pressure offset of +2.5 Pa to +5 Pa. When the theatre doors open, sterile air violently pushes outward, creating an invisible, physical shield against corridor contaminants.
- The Metric: The system guarantees the mandatory 20–25 air changes per hour (ACH), refreshing the room with 100% HEPA-filtered air every few minutes.
Use Case 2: The Infectious Disease Isolation Ward (Negative Pressure)
- The Problem: Aerosolised viruses must be contained within the patient’s room to protect hospital staff and immunocompromised patients in adjacent wards.
- The AHU Outcome: The AHU room is engineered to extract 15–20% more air than it supplies, creating a vacuum effect.
- The Metric: The AHU safely exhausts contaminated air outdoors, above the roofline, maintaining a continuous negative pressure differential of -2.5 Pa.
The Comparison: Commercial HVAC vs Hygienic Hospital AHUs
Many hospitals fail audits because procurement opted for standard commercial AHUs to save CapEx. In a healthcare setting, standard units degrade rapidly under the strain of high static pressure and continuous run-times.
Here is why upgrading to a custom Class L1 hygienic unit (like those engineered by AADtech) is a regulatory necessity.
| Head-to-Head Comparison Table | Standard Commercial AHU | Custom Hygienic (Class L1) AHU |
| Casing Leakage | Class L3 (Allows bypass air) | Class L1 (Zero-leakage): Ensures 100% of air passes through HEPA filters, eliminating “Phantom Bypass”. |
| Drainage / Hygiene | Flat galvanised pans | Sloped stainless steel trays: Eliminate stagnant water and remove breeding grounds for Legionella. |
| Audit Accessibility | Screwed access panels | Fitted DOP-test ports: Reduces filter-validation testing from four hours to under ten minutes, ensuring Phantom Bypass can be detected and eliminated instantly. |
| Acoustic Control | Single skin, basic mounts | Thermal-acoustic breaks: Keep ward noise below 35 dB(A) to lower cortisol and accelerate ICU recovery. |
| Lifespan | 5 to 7 years | 15+ years: Prevents costly late-life AHU replacement in active wards. |
Pros and Cons of Investing in Custom Hygienic AHUs
If you are pitching a plant room upgrade to the C-suite, you must present a balanced, ROI-driven business case.
The Pros:
- Audit insurance: Guarantees compliance with HTM 03-01 and ASHRAE 170 by enforcing a Class L1, zero-leakage casing, and eliminating the risk of forced ward closures.
- Total infection control: Class L1 double-skin casing means zero unfiltered air reaches the patient.
- Operational efficiency: Integrated UV-C lamps automatically destroy cooling-coil biofilms, drastically reducing the hours your maintenance team spends on manual deep cleaning.
The Cons (And How to Mitigate Them):
- Higher initial CapEx: Custom units cost 20–40% more upfront than off-the-shelf commercial boxes. (Mitigation: The ROI is typically achieved within three years via energy savings, extended filter life, and reduced maintenance downtime.
- Increased weight: Hygienic double-skin stainless steel units are heavy. (Mitigation: Structural engineers from bodies like IHEEM must verify plant room slab load-bearing limits before installation.
- Longer lead times: Because they are custom-built to specific ward pressure metrics, manufacturing takes longer. (Mitigation: Factor a 12–16 week lead time into the renovation programme).
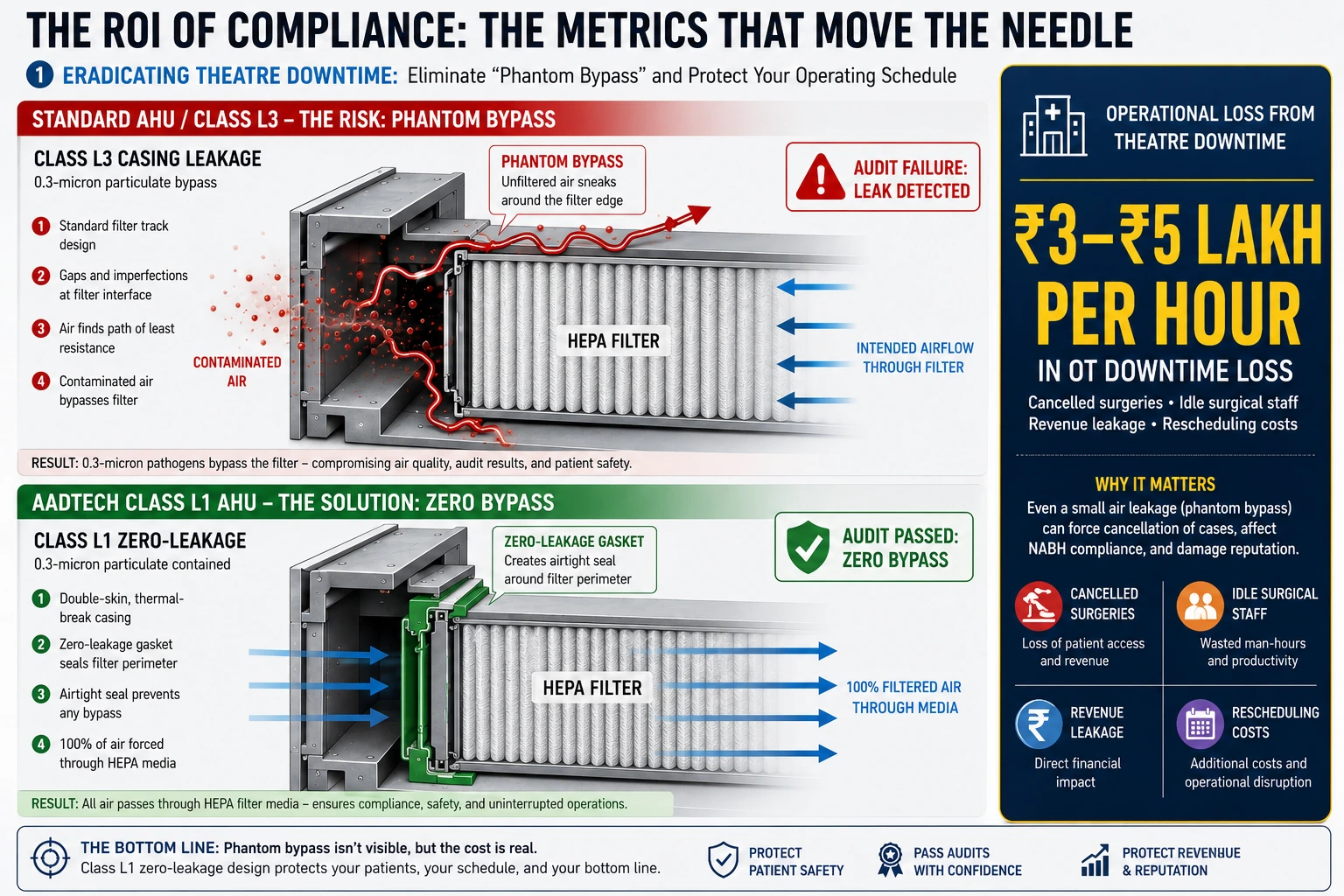
The ROI of Compliance: The Metrics That Move the Needle
Upgrading an AHU room is not a sunk cost; it is a high-yield operational and clinical investment.
1. Eradicating Theatre Downtime (Risk Mitigation)
If an auditor finds a HEPA bypass leak, they will shut the surgical theatre down immediately. The average cost of a cancelled operating-theatre schedule is roughly ₹3 lakh–₹5 lakh in lost revenue and wasted surgical-staff time per hour. A bespoke, zero-leakage AHU acts as an insurance policy against this catastrophic financial loss.
Source: NHS England (Health Technical Memorandum 03-01)
2. The 30% Energy Reclamation (OpEx Reduction)
Historically, hospital AHUs relied on Constant Air Volume (CAV) systems. It is running fans at 100% capacity even when the theatre was empty at 3:00 AM. By integrating Variable Air Volume (VAV) boxes with smart BMS sensors, a modern AHU reduces fan speeds during unoccupied hours while maintaining the legal baseline pressure. This intelligent setback strategy reduces HVAC energy consumption by up to 30% annually, directly supporting hospital decarbonisation targets.
3. Extending Motor and Filter Lifespan
When pre-filters bypass air, HEPA filters clog faster. It thus forces the AHU fan motor to work harder to maintain the required air changes per hour, calculated during validation as:
$$ACH = \frac{Q \times 3600}{V}$$
By ensuring airtight pre-filtration, custom units can extend HEPA-filter life from six months to 18 months, while doubling the lifespan of the VFD motors.
Final Verdict: Move Forward, Don’t Just Maintain
You cannot solve healthcare-grade infection control with commercial-grade sheet-metal casings. The AHU room serves as an impenetrable physical barrier between your vulnerable patients and airborne pathogens.
If your current AHU casing leaks, your pressure offsets fluctuate, or your noise levels extend patient recovery times, your facility is already failing its most critical function. Stop repairing non-compliant systems. Partner with technical specialists at AADtech to audit your current plant room, calculate your bypass leakage rates, and design a Class L1 hygienic upgrade that guarantees your hospital’s safety, compliance, and financial efficiency for two decades.
Frequently Asked Questions
Under HTM 03-01 guidelines, an orthopaedic operating theatre requires a minimum of 20-25 air changes per hour (ACH) to dilute and remove airborne contaminants from the sterile field rapidly.
The AHU room prevents infections by supplying terminal HEPA-filtered air, creating a positive-pressure environment (+2.5 Pa to +5 Pa). This physical pressure barrier prevents contaminated corridor air from entering the operating theatre during surgery.
A standard commercial AHU allows for acceptable levels of air leakage (Class L3) and uses basic drainage pans. A hygienic medical-grade AHU utilises a zero-leakage Class L1 casing to prevent “Phantom Bypass,” alongside sloped stainless steel drain trays to prevent Legionella and biofilm growth.
According to HTM 03-01 Part B, specialised healthcare ventilation systems must undergo formal verification and validation (V&V) at least annually. It includes mandatory DOP (Dispersed Oil Particulate) testing to ensure HEPA filters have zero bypass leakage.
AHU rooms must integrate with the hospital’s fire alarm matrix and feature motorised fire and smoke dampers within the ductwork. Upon detecting smoke, the system must either safely extract it or shut down entirely to prevent toxic fumes from circulating into patient recovery wards.
Reference List
- ASHRAE Standard 170 – Ventilation of Health Care Facilities
- NHS England – HTM 03-01 Specialised Ventilation for Healthcare Premises
- Centres for Disease Control and Prevention (CDC) – Guidelines for Environmental Infection Control in Healthcare Facilities
- IHEEM – Institute of Healthcare Engineering and Estate Management
- World Health Organisation (WHO) – Natural Ventilation for Infection Control in Healthcare Settings
- NABH – National Accreditation Board for Hospitals & Healthcare Providers
- ASHRAE Journal – Healthcare Ventilation and Pressure Relationships